
Page Contents
1. Introduction of the Complexity of Spinal Cord Injuries (SCI)
Spinal cord injury (SCI) represents one of the most debilitating conditions in modern medicine, often resulting in permanent motor, sensory, and autonomic dysfunction below the site of injury. Each year, an estimated 250,000 to 500,000 people worldwide suffer from SCI, primarily due to trauma from vehicle accidents, falls, or sports injuries. The pathophysiology of SCI includes both primary mechanical damage and secondary processes such as inflammation, oxidative stress, and apoptosis. The limited regenerative capacity of the central nervous system (CNS) poses a significant barrier to recovery, prompting the need for innovative therapeutic strategies. Among emerging modalities, laser therapy, also known as photobiomodulation (PBM), has gained attention for its potential to modulate cellular and molecular mechanisms crucial to neuronal survival and repair. This blog delves into the scientific basis, therapeutic benefits, clinical evidence, and integration of laser therapy into SCI rehabilitation, grounded in recent peer-reviewed research and medical consensus.
2. Laser Therapy Explained: Mechanism and Modalities
Laser therapy is a non-invasive treatment that uses specific wavelengths of light to stimulate biological processes. For spinal cord injury (SCI), laser therapy—especially photobiomodulation—has emerged as a potential adjunct treatment that targets cellular mechanisms involved in repair, inflammation, and neuroregeneration. This section delves into the types of laser therapy, the science behind photobiomodulation, the key molecular pathways it influences, and its safety profile.
2.1 Types of Laser Therapy
Laser therapy for SCI can be categorized into two types based on power output, wavelength, and therapeutic goals. Low-Level Laser Therapy (LLLT), also known as cold laser or photobiomodulation therapy (PBMT), uses low-intensity light within the red and near-infrared spectrum (typically 600–1000 nm). LLLT is non-thermal, meaning it does not produce heat, and is designed to stimulate cellular processes. It is the most studied modality in neurological applications and is associated with anti-inflammatory, anti-apoptotic, and neuroregenerative effects. Unlike LLLT, High-Intensity Laser Therapy (HILT) uses higher-powered lasers (>500 mW) and may generate thermal effects. Its use in neurological rehabilitation is more cautious due to the risk of tissue heating but can penetrate deeper tissues, which is beneficial for treating muscular pain or deep-seated lesions in combination with other methods.
2.2 How Photobiomodulation Works
Photobiomodulation (PBM) works by applying specific light wavelengths that penetrate tissues and are absorbed by chromophores, most notably cytochrome c oxidase (CCO) in the mitochondria. The interaction leads to several downstream biological effects:
- Increased ATP Production: Light absorption enhances mitochondrial respiration, leading to elevated levels of adenosine triphosphate (ATP), the energy currency of the cell. ATP is critical for cell survival, repair, and regeneration, especially in metabolically compromised neurons post-injury.
- Modulation of Reactive Oxygen Species (ROS): Controlled production of ROS acts as signaling molecules, activating transcription factors and promoting cellular repair. While excessive ROS can be damaging, PBM induces ROS within a therapeutic window.
- Nitric Oxide (NO) Release: PBM promotes vasodilation through nitric oxide release, improving local blood flow and oxygen delivery to ischemic tissues.
- Altered Gene Expression: PBM influences the expression of genes involved in inflammation, apoptosis, and neurogenesis. Key transcription factors such as NF-κB, HIF-1α, and Nrf2 are modulated to create a pro-healing microenvironment.
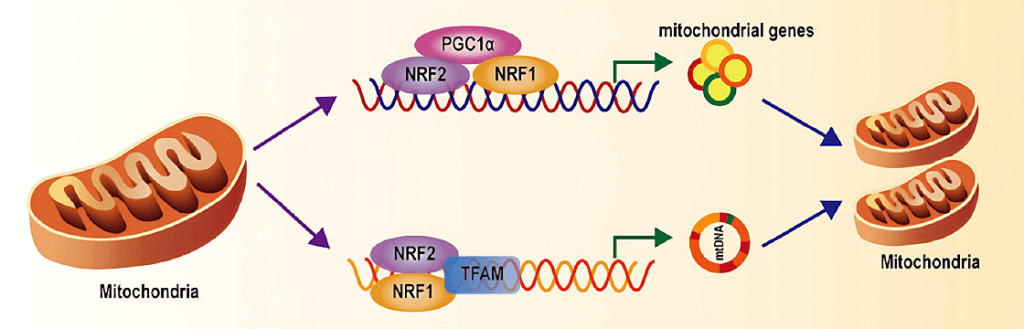
2.3 The AMPK/PGC-1α/TFAM Pathway: Mitochondrial Repair in Neurons
Recent research highlights the importance of the AMPK/PGC-1α/TFAM pathway in mediating PBM’s therapeutic effects on neurons. AMPK (AMP-Activated Protein Kinase) is a cellular energy sensor that activates when energy levels are low. PBM activates AMPK, which in turn initiates catabolic processes that generate ATP while inhibiting anabolic pathways that consume energy. PGC-1α (Peroxisome Proliferator-Activated Receptor Gamma Coactivator 1-alpha) is a transcriptional coactivator induced by AMPK. It promotes mitochondrial biogenesis, increases antioxidant enzyme expression, and improves metabolic efficiency. TFAM (Mitochondrial Transcription Factor A) regulates mitochondrial DNA (mtDNA) replication and transcription. Its expression, upregulated by PGC-1α, is crucial for mitochondrial repair and the synthesis of mitochondrial proteins essential for ATP production. Activation of this pathway through PBM in SCI models leads to improved mitochondrial integrity, enhanced neuronal survival, and greater resilience against secondary injury processes such as inflammation and apoptosis.
2.4 Safety Profile of Laser Therapy
Laser therapy, particularly LLLT, is generally well-tolerated and considered safe when administered correctly. LLLT does not heat tissues, making it safe for neural structures. Its application is painless and does not require surgical intervention. Reported side effects are rare and typically minor, such as mild skin redness, tingling, or warmth at the treatment site. There are no known systemic side effects. Laser therapy should be avoided over active cancerous lesions, the thyroid gland, the pregnant uterus, and directly over the eyes. Patients with photosensitivity disorders should also be evaluated carefully. Clinical studies consistently report a high safety margin for PBM, but professional training and adherence to guidelines are critical to ensuring its safe application.
3. Evidence-Based Benefits of Laser Therapy for SCI
Photobiomodulation (PBM), commonly known as laser therapy, has emerged as a compelling adjunct in neurorehabilitation, particularly in the context of spinal cord injury (SCI). Its appeal lies in its ability to interact at the cellular level to promote survival, repair, and regeneration of nervous tissue. SCI results in not only the immediate disruption of spinal cord pathways but also a cascade of secondary damage, including inflammation, oxidative stress, and cell death. PBM—especially in the red to near-infrared (NIR) spectrum (600–980 nm)—has shown the capacity to modulate these pathological responses. The benefits of laser therapy are multifaceted and interdependent, offering promise for both acute management and chronic recovery in SCI patients.
3.1 Enhancing Neuronal Survival and Growth
One of the most crucial therapeutic goals after spinal cord injury is to protect neurons from apoptosis and encourage the regrowth of damaged neural tissue. PBM contributes to this goal by activating key pro-survival signaling pathways such as the PI3K/Akt and ERK1/2 cascades. These pathways are instrumental in upregulating anti-apoptotic proteins like Bcl-2 while simultaneously suppressing pro-apoptotic markers such as caspase-3. In parallel, PBM influences the expression of neurotrophic factors including Brain-Derived Neurotrophic Factor (BDNF) and Nerve Growth Factor (NGF), both of which are essential for stimulating neurogenesis and supporting neurite extension. In the structural context, PBM also appears to facilitate axonal regeneration by stabilizing microtubules and reorganizing extracellular matrix components, which are often degraded following trauma. Together, these effects contribute to a more favorable environment for neuronal preservation and regrowth.
3.2 Improving Functional Recovery
Beyond cellular protection, PBM has been associated with tangible improvements in motor and sensory function—key indicators of recovery after SCI. This is largely due to its role in promoting remyelination. PBM stimulates the proliferation and maturation of oligodendrocyte precursor cells, which are responsible for restoring the insulating myelin sheath around axons. This remyelination is crucial for re-establishing efficient electrical conduction along spinal pathways. Additionally, PBM enhances synaptic plasticity by influencing the expression of synapsin and the density of dendritic spines, thereby aiding the reformation of damaged neural circuits. Improved neurovascular coupling—an increase in blood flow and oxygen delivery to regenerating tissue—further supports functional restoration. These cellular and vascular benefits translate into improved outcomes in animal models, where PBM-treated rodents exhibit superior scores on locomotor assessments like the Basso, Beattie, and Bresnahan (BBB) scale. Such improvements include better hind-limb coordination, reduced gait abnormalities, and more balanced postural control.
3.3 Reducing Inflammation and Oxidative Stress
Inflammation and oxidative stress are two of the most damaging secondary consequences of SCI, and both are effectively modulated by PBM. After injury, the spinal cord becomes inundated with pro-inflammatory cytokines such as TNF-α and IL-1β, as well as reactive oxygen species (ROS), which further damage neurons and glial cells. PBM helps break this vicious cycle by downregulating the activity of NF-κB, a transcription factor that drives the expression of numerous pro-inflammatory genes. Simultaneously, it upregulates the body’s own antioxidant defense systems, increasing the activity of enzymes like superoxide dismutase (SOD) and glutathione peroxidase (GPx). These antioxidants help neutralize harmful free radicals and reduce lipid peroxidation, thus protecting cellular membranes and mitochondrial integrity. Moreover, PBM modulates microglial behavior, shifting their phenotype from M1 (pro-inflammatory) to M2 (anti-inflammatory), which creates a regenerative environment more conducive to healing and tissue repair.
3.4 Supporting Mitochondrial Health
The role of mitochondria in SCI is often underestimated, but mitochondrial dysfunction is central to the injury’s progression. Energy deficits, oxidative damage, and apoptosis all stem in part from impaired mitochondrial function. PBM targets this problem directly by acting on cytochrome c oxidase (Complex IV) in the electron transport chain, thereby boosting ATP production and restoring cellular energy balance. It also activates the AMPK/PGC-1α/TFAM pathway, which governs mitochondrial biogenesis and the transcription of mitochondrial DNA, ensuring that damaged cells have the means to regenerate energy-producing organelles. Furthermore, PBM helps stabilize the mitochondrial membrane potential, reducing the risk of cytochrome c release into the cytosol—a key trigger of intrinsic apoptosis. Through these mechanisms, laser therapy strengthens the energy infrastructure of injured cells, empowering them to survive and function even in the face of traumatic insult.

4. Clinical Evidence & Research Insights
Although laser therapy—particularly photobiomodulation (PBM)—has shown considerable promise in laboratory settings, its application in clinical rehabilitation for spinal cord injury (SCI) is still in early phases. Nonetheless, both preclinical and emerging clinical studies offer meaningful insights into how laser therapy might revolutionize SCI management. The research so far suggests significant neuroprotective and regenerative potential, but more robust clinical validation is needed. This section outlines the core findings from rodent models, early-stage human trials, and the current limitations shaping future research directions.
4.1 Preclinical Studies in Rodents
Animal studies, particularly in rodent models of spinal cord injury (SCI), strongly support the potential of laser therapy. Rats treated with transcutaneous photobiomodulation (PBM) after SCI showed more surviving neurons near the lesion and performed better on locomotor tests like the BBB scale, indicating improved motor recovery. Histological analysis confirmed smaller lesion volumes, fewer cystic cavities, and better white matter preservation. These structural improvements suggest enhanced spinal cord integrity. Notably, the timing and dosage of PBM were crucial—initiating treatment within 24 to 72 hours post-injury and using wavelengths between 800 and 850 nm yielded the best results. These findings highlight PBM’s ability to reduce secondary damage, support axonal regrowth, and speed up functional recovery when precisely applied.
4.2 Human Clinical Applications (Early-Stage)
Though human clinical trials are limited, early findings suggest laser therapy may aid spinal cord injury (SCI) recovery. Preliminary studies report modest improvements in neurological function, with some patients improving from complete (ASIA grade A) to incomplete injuries (grades B or C). Case reports also show notable reductions in neuropathic pain, a common and hard-to-treat symptom in chronic SCI. Beyond pain relief, patients have reported benefits such as reduced spasticity, better mobility, and improved bladder control. Importantly, no serious side effects have been observed, highlighting the treatment’s safety. These initial results are promising, but larger, controlled studies are needed to confirm laser therapy’s effectiveness and define standardized treatment guidelines.
4.3 Limitations and Research Gaps
Several challenges limit the broader adoption of laser therapy for spinal cord injury (SCI). Chief among them is the lack of standardized treatment protocols—studies differ in wavelength, dosage, and frequency, complicating comparison. Promising rodent studies don’t easily translate to human physiology, and the number of human randomized controlled trials (RCTs) remains small. While mitochondrial and anti-inflammatory mechanisms are suggested, the full molecular effects of laser therapy aren’t fully understood. Long-term outcomes are also unclear, as many studies lack extended follow-up. To move forward, multicenter RCTs, detailed biomarker research, and personalized protocols based on injury type and patient characteristics are essential.
5. Integration into Rehabilitation Protocols
Laser therapy is most effective when thoughtfully integrated into a broader multidisciplinary rehabilitation program for SCI. Optimal outcomes depend on appropriate timing, individualized dosing, synergy with adjunct therapies, and careful selection of treatment platforms.
5.1 Timing and Dosage Considerations
Timing plays a vital role in spinal cord injury (SCI) recovery, as each phase—acute, subacute, and chronic—offers unique treatment opportunities. In the acute phase (within 48 hours), early photobiomodulation (PBM) may reduce inflammation and secondary damage, especially if started within 6–12 hours post-injury. During the subacute phase, laser therapy supports axonal repair and new blood vessel growth. In the chronic phase, PBM helps maintain function, reduce pain, and boost neuroplasticity. Proper dosing is key: effective parameters typically use wavelengths of 800–980 nm, power densities of 10–1000 mW/cm², and fluences of 4–10 J/cm². Treatments last 30 seconds to 2 minutes per point and target the injured spinal segments regularly.
5.2 Combining Laser Therapy with Other Modalities
Laser therapy serves as a powerful adjunct within multimodal SCI rehabilitation protocols. When combined with physical therapy and functional electrical stimulation (FES), PBM can enhance muscle responsiveness, reduce spasticity, and improve range of motion. Integrating PBM with pharmacological agents—such as anti-inflammatory drugs or neuroprotective compounds—may enhance both systemic and localized effects. Furthermore, PBM can improve the therapeutic yield of stem cell therapies by modulating the injury microenvironment to promote cell survival, homing, and integration. Advanced rehabilitation tools like robotic gait training and exoskeletons can also benefit from concurrent PBM sessions by improving neuromuscular activation and endurance. The synergistic potential of PBM with these therapies underscores the need for individualized, coordinated treatment plans that leverage the multifaceted benefits of laser intervention.

5.3 At-Home and Clinical Device Options
Laser therapy is increasingly available through both clinical-grade systems and consumer-friendly home-use devices. Class IV lasers, typically used in clinical settings, offer higher power outputs (>500 mW), allowing deeper penetration and broader treatment coverage. These systems require professional operation and are typically employed in specialized rehabilitation centers. On the other hand, Class IIIb devices (power <500 mW) or LED-based photobiomodulation tools are designed for home use, offering lower power but greater convenience. These are especially suitable for chronic maintenance or superficial application. Safety features, preset dosing protocols, and ergonomic designs make them accessible for patients with limited mobility. However, users must receive adequate training and follow physician guidance to ensure safe and effective treatment. The choice between clinical and home-based PBM systems should be informed by the injury’s severity, treatment goals, and patient capabilities.
6. Expert Opinions & Ethical Considerations
Experts in neurorehabilitation see laser therapy as a valuable tool for spinal cord injury (SCI) care. Dr. Juanita Anders, a leader in photobiomodulation research, highlights its ability to influence cell metabolism and inflammation without drug side effects. Still, ethical concerns persist. Overcommercialization may lead vulnerable SCI patients to fall for unproven “miracle cure” claims from unregulated sources. Clear communication about realistic outcomes is essential. Access is also an issue—many patients in low-resource areas may lack quality devices or trained providers. Since PBM use is still evolving, clinicians must ensure informed consent and explain the experimental nature of treatment. Ethical practice calls for evidence-based care, ongoing education, and prioritizing patient well-being over profit.
7. Summary
Laser therapy represents a rapidly evolving adjunctive treatment for spinal cord injury rehabilitation. Photobiomodulation, particularly within the near-infrared spectrum (800–980 nm), targets key mechanisms involved in secondary SCI pathology. It has demonstrated the ability to reduce inflammation, protect mitochondria, enhance neuronal survival, and stimulate axonal regeneration. Preclinical studies have consistently shown benefits in animal models, with early-stage human trials revealing improvements in pain, motor function, and overall quality of life. Importantly, PBM offers a non-invasive, safe, and well-tolerated option for SCI patients across different stages of recovery. When integrated with physical therapy, pharmacological treatments, and assistive technologies, laser therapy can amplify therapeutic gains and facilitate functional restoration. Despite current research limitations, the future of laser therapy in SCI rehabilitation appears promising. Ongoing clinical trials and technological innovation will likely shape its role as a standard of care in neurorehabilitation.
8. FAQs about Laser Therapy for SCI
Q1: Does laser therapy cause any side effects?
Laser therapy is generally considered safe. Most reported side effects are mild and transient, such as localized warmth or slight redness. No serious adverse effects have been documented in SCI trials.
Q2: How soon after injury should laser therapy be started?
Early initiation—ideally within the first 24–72 hours—may yield the most significant neuroprotective benefits. However, benefits can also be seen during subacute and chronic stages, particularly for pain reduction and motor support.
Q3: Can I use a laser device at home?
Yes. Certain Class IIIb PBM devices are designed for home use and are effective for chronic pain and maintenance therapy. Always consult a physician before starting home treatment to ensure safety and proper dosing.
Q4: Is laser therapy a cure for SCI?
No. Laser therapy is not a cure but a supportive modality that can enhance the efficacy of other treatments and promote functional recovery.
Q5: Can laser therapy help with spasticity or bladder control?
Preliminary reports suggest some improvements in spasticity and autonomic functions, including bladder sensation. However, further clinical validation is needed.
Q6: How long is a typical treatment session?
Treatment durations vary by protocol but generally range from 10 to 30 minutes per session, depending on the size of the treatment area and the laser’s parameters.
9. References
A Review of Low-Level Laser Therapy for Spinal Cord Injury: Challenges and Safety:
https://pmc.ncbi.nlm.nih.gov/articles/PMC7736940
Role of Low-Level Laser Therapy in Neurorehabilitation:
https://www.sciencedirect.com/science/article/abs/pii/S1934148210012530
Photobiomodulation promotes repair following spinal cord injury by restoring neuronal mitochondrial bioenergetics via AMPK/PGC-1α/TFAM pathway:
https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2022.991421/full