
Conteúdo da página
Introdução
Upper limb spasticity is a common and debilitating complication following a stroke, limiting functional independence, reducing quality of life, and complicating daily activities such as dressing, eating, and personal hygiene. Traditional management strategies include physical therapy, oral medications, and sometimes invasive procedures like botulinum toxin injections or surgery. Class IV laser therapy offers a non-invasive adjunctive approach that leverages high-intensity light energy to penetrate soft tissues, modulate cellular activity, improve microcirculation, and support muscle relaxation. Emerging clinical evidence suggests that incorporating Terapia laser de classe IV into comprehensive rehabilitation plans may enhance functional outcomes, reduce pain, and improve overall patient engagement in recovery.
1. Understanding Post-Stroke Upper Limb Spasticity
Before exploring treatment options, it is essential to understand the pathophysiology of post-stroke spasticity and its impact on upper limb function.
1.1 Pathophysiology of Spasticity
Spasticity occurs due to upper motor neuron lesions following ischemic or hemorrhagic strokes. Damage to corticospinal tracts leads to an imbalance in excitatory and inhibitory signals, resulting in increased muscle tone, hyperreflexia, and involuntary contractions. In upper limbs, this often affects the flexor muscles of the forearm and hand, causing a flexed posture and restricted range of motion. Chronic spasticity can lead to secondary complications such as contractures, joint deformities, and skin breakdown in severe cases. Understanding these mechanisms highlights the importance of early intervention to prevent long-term disability.
1.2 Functional Implications
Spasticity severely limits daily activities, from grasping objects to performing self-care tasks. Patients may experience persistent pain due to muscle overactivity and ischemia, further discouraging use of the affected limb. Reduced mobility can also contribute to secondary musculoskeletal issues, such as shoulder subluxation or muscle atrophy, emphasizing the need for therapies that address both neural and musculoskeletal components of spasticity.
2. Mechanisms of Class IV Laser Therapy
Class IV laser therapy employs high-intensity infrared light (typically 10–15 W) capable of penetrating several centimeters into soft tissue, stimulating cellular responses without causing thermal damage.
2.1 Photobiomodulation and Cellular Activity
Class IV lasers induce photobiomodulation, a process in which light energy is absorbed by chromophores in mitochondria, leading to increased ATP production, enhanced cellular metabolism, and modulation of inflammatory mediators. In post-stroke muscles, these effects may reduce localized inflammation, improve mitochondrial function, and promote tissue repair. By enhancing cellular energy availability, laser therapy can support both neural and muscular recovery mechanisms.
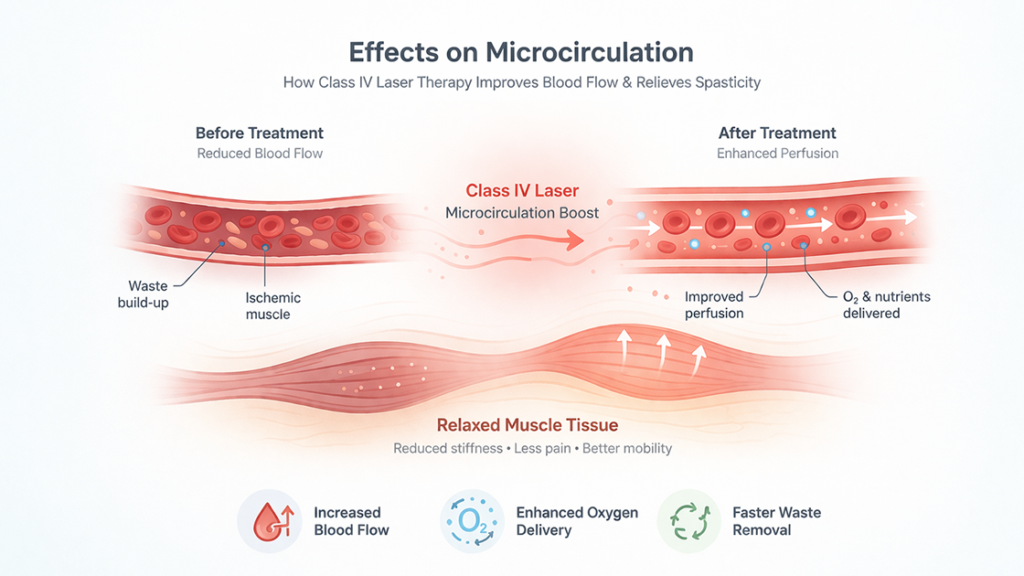
2.2 Effects on Microcirculation
One critical mechanism of Class IV laser therapy is its ability to enhance local blood flow and microcirculation. Increased perfusion delivers oxygen and nutrients to ischemic or hypertonic muscles, helping alleviate pain and reducing stiffness. Improved circulation also facilitates waste removal, supporting metabolic recovery in chronically spastic muscles.
2.3 Neuromuscular Modulation
Laser therapy may influence nerve conduction and neuromuscular excitability. Studies suggest that photobiomodulation can reduce hyperactive reflex arcs, potentially decreasing muscle tone in spastic regions. While the exact neural mechanisms remain under investigation, the observed functional improvements in clinical settings indicate a meaningful impact on upper limb motor control.
3. Clinical Evidence for Upper Limb Spasticity
Several clinical studies have investigated the efficacy of Class IV laser therapy for post-stroke spasticity, particularly in combination with conventional rehabilitation.
3.1 Randomized Controlled Trials
RCTs have demonstrated that patients receiving Class IV laser therapy alongside physical therapy exhibit statistically significant reductions in Modified Ashworth Scale scores compared to controls. Improvements are typically observed in wrist, forearm, and hand flexor muscles, with better passive and active range of motion. These findings suggest that laser therapy can complement existing rehabilitation protocols by enhancing motor recovery.
3.2 Functional Outcomes
Beyond tone reduction, studies report improved functional performance in activities of daily living (ADLs). Patients often regain the ability to grasp and release objects, improve hand positioning, and participate more actively in self-care tasks. These functional gains translate to greater independence and quality of life, highlighting the real-world benefits of integrating Class IV laser therapy into post-stroke care.
3.3 Safety Profile
Class IV laser therapy is generally well tolerated. Adverse events are rare and typically limited to transient warmth or mild erythema at the application site. Unlike invasive interventions, there is no risk of infection or systemic side effects, making it a suitable adjunct for patients who may not tolerate medications or injections well.
4. Integration with Rehabilitation Strategies
For optimal results, Class IV laser therapy is most effective when combined with conventional rehabilitation modalities.
4.1 Physical and Occupational Therapy
Laser therapy can enhance the effects of stretching, range-of-motion exercises, and task-specific training. By reducing muscle hypertonicity, it allows therapists to achieve greater joint mobility and more effective strengthening exercises. Patients often experience reduced pain during therapy sessions, which encourages active participation and compliance.
4.2 Timing and Frequency
Treatment protocols typically involve multiple sessions per week, with each session lasting 10–20 minutes per muscle group, depending on severity and patient tolerance. Clinicians adjust parameters such as wavelength, power output, and pulse frequency to maximize therapeutic effects while minimizing discomfort.
4.3 Complementary Approaches
Other complementary interventions, including neuromuscular electrical stimulation, splinting, or pharmacological agents, can be used alongside laser therapy. This multimodal approach addresses both the neurological and musculoskeletal components of spasticity, promoting sustained functional improvement.
5. Patient Selection and Considerations
Not all post-stroke patients are ideal candidates for Class IV laser therapy.
5.1 Inclusion Criteria
Patients with mild-to-moderate spasticity who can tolerate laser exposure and have sufficient soft tissue coverage benefit most. Early intervention post-stroke may yield better outcomes by preventing contracture formation and muscle shortening.
5.2 Contraindications
Class IV laser therapy should be used cautiously or avoided in patients with malignancies in the treatment area, photosensitivity disorders, or active infections. Clinicians also consider comorbidities such as cardiovascular instability or skin conditions that may increase sensitivity to light therapy.
5.3 Realistic Expectations
While laser therapy can reduce spasticity and improve function, it is not a cure for the underlying neurological injury. Patients and caregivers should understand that sustained improvements require ongoing rehabilitation, and laser therapy serves as an adjunct to conventional therapies rather than a standalone solution.
FAQ
Q1: How soon can patients see improvements after Class IV laser therapy?
A1: Many patients report reduced muscle stiffness and improved movement within a few sessions, though full functional gains typically require several weeks of combined therapy.
Q2: Is Class IV laser therapy painful?
A2: The treatment is generally painless; patients may feel mild warmth or tingling at the application site.
Q3: Can it be used on all stroke patients?
A3: It is most effective in patients with mild-to-moderate spasticity; severe contractures may require additional interventions.
Q4: How often should therapy be administered?
A4: Typical protocols involve 2–5 sessions per week, depending on severity and clinician guidance.
Q5: Are there any long-term side effects?
A5: Adverse effects are rare; most patients tolerate the therapy well with transient warmth being the most common reaction.
Conclusão
Class IV laser therapy represents a promising non-invasive adjunct for managing post-stroke upper limb spasticity. By modulating neuromuscular activity, enhancing microcirculation, and promoting tissue repair, it can reduce muscle hypertonicity and support functional recovery. When integrated into comprehensive rehabilitation plans alongside physical and occupational therapy, it offers meaningful improvements in range of motion, pain reduction, and independence. While it is not a standalone cure, its safety profile and efficacy make it a valuable tool in optimizing post-stroke rehabilitation outcomes.
References
Alayat MS, et al. Effect of high-intensity laser therapy on post-stroke spasticity: A randomized controlled trial. Lasers Med Sci. 2014;29:1737–1743.
https://pubmed.ncbi.nlm.nih.gov/24509716/
Dos Santos GM, et al. Photobiomodulation in upper limb spasticity after stroke: A systematic review. J Stroke Cerebrovasc Dis. 2019;28:104338.
https://pubmed.ncbi.nlm.nih.gov/30902402/
Khalili H, et al. High-intensity laser therapy combined with physical therapy in post-stroke spasticity. J Rehabil Med. 2018;50:708–716.
https://pubmed.ncbi.nlm.nih.gov/30040828/
Bjordal JM, et al. Mechanisms and clinical effects of low and high-intensity laser therapy in musculoskeletal disorders. Photomed Laser Surg. 2006;24:235–246.
https://pubmed.ncbi.nlm.nih.gov/16941236/
Duarte JA, et al. Class IV laser therapy for spasticity reduction and functional improvement: A clinical perspective. Lasers Surg Med. 2020;52:183–191.