
ページ内容
はじめに
A boxer takes a hard hook to the jaw. His head whips sideways, and for a split second, his neck feels like it stretched too far. A rugby player gets tackled from an angle she didn‘t come from. Her cervical spine twists violently, and afterward, something just feels off. Weeks later, the neck pain lingers. Headaches appear after every practice. Rotating the head feels locked or painful. These athletes may be dealing with something more than a simple muscle strain—they may have injured their alar ligaments. The alar ligaments are small but critically important structures deep inside the upper neck that control how much the head rotates and bends sideways. When these ligaments stretch or tear, the result is not just pain but a subtle instability that can derail an athletic career. This article explains why boxers and rugby players face high risks for alar ligament strains, how Class IV laser therapy promotes healing in this hard-to-reach region of the cervical spine, and how athletes can integrate laser treatment into a comprehensive return-to-sport plan.
1. Understanding the Alar Ligament and Its Role in Contact Sports
The alar ligaments sit deep inside the craniocervical junction—the complex region where the skull meets the top two vertebrae of the spine. For athletes in high-impact contact sports, these ligaments face forces far beyond what the average person ever experiences.
1.1 Anatomy and Function of the Alar Ligaments
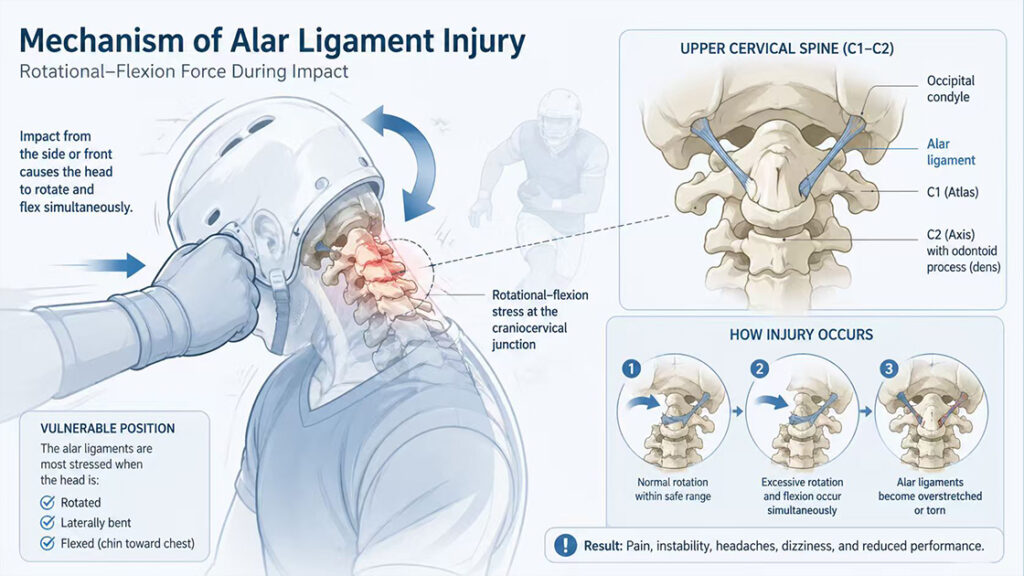
The alar ligaments are paired cord‑like structures that connect the odontoid process (dens) of the second cervical vertebra (C2) to the occipital condyles at the base of the skull. Shaped like two small wings, each ligament measures approximately 10–13 mm in length. Their primary job is to limit excessive rotation and lateral bending of the head. When you turn your head to the left, the right alar ligament tightens to prevent over‑rotation. This braking mechanism protects the spinal cord and surrounding nerves from being stretched or crushed. Without properly functioning alar ligaments, the upper cervical spine becomes unstable, and every head movement carries risk.
1.2 How Contact Sports Damage the Alar Ligaments
Alar ligament injuries typically result from high‑velocity trauma that forces the head and neck into an extreme range of motion. In boxing, this happens when a punch strikes the jaw or temple, snapping the head sideways. The mechanism that most strains the alar ligaments occurs when the head is both rotated and flexed (bent forward) at the same time. A rugby player driving into a tackle often enters this exact vulnerable position. Whiplash‑type forces during tackles or falls also damage these ligaments considerably. Unlike muscles, which heal relatively quickly, ligaments consist mainly of collagen fibers that recover slowly and often incompletely.
1.3 Subtle Symptoms Athletes Often Ignore
Alar ligament injuries do not always announce themselves with dramatic pain. More often, athletes report a dull, deep ache near the base of the skull on one side. The pain worsens when rotating the head to the injured side or when looking upward. Some athletes describe a heavy head feeling, as if their neck muscles cannot properly hold up the skull. Headaches that start at the back of the head and spread forward are also common, along with occasional dizziness or a sense of imbalance. A boxer may notice that his reaction time feels slightly off. A rugby player may find that tracking a moving ball during a play causes disorientation. These are not signs of simple muscle soreness.
2. Class IV Laser Therapy – How It Reaches Deep Ligament Tissue
Standard cold laser therapy (Class IIIB) penetrates only superficial tissues. Class IV laser therapy operates at much higher power levels, delivering enough energy to reach ligaments buried several centimeters beneath muscles, fascia, and bone.
2.1 What Makes Class IV Different from Cold Lasers
Class IV lasers are defined as therapeutic lasers with output power exceeding 500 mW. Many clinical devices operate at 15W, 30W, or even 60W of power. This higher power allows the near‑infrared wavelengths (typically 810 nm to 1064 nm) to penetrate up to 5–7 cm deep into tissue. For comparison, a standard cold laser penetrates only 1–2 cm. That difference matters greatly for the alar ligaments, which sit deep within the upper cervical spine, surrounded by thick layers of paraspinal muscles. Only a high‑power laser can deliver therapeutic photons to that depth.
2.2 The Photobiomodulation Mechanism for Ligament Healing
When near‑infrared light reaches the damaged ligament, cells called fibroblasts absorb photons through their mitochondria. This energy boosts adenosine triphosphate (ATP) production and triggers a cascade of healing responses. The laser accelerates collagen synthesis, which directly supports the repair of the alar ligament‘s collagen fibers. It reduces levels of inflammatory mediators like TNF‑α and IL‑6, lowering local inflammation without drugs. By activating fibroblasts and supporting tissue regeneration, the therapy creates an environment where the slow‑healing ligament can finally repair itself. Patients typically experience the laser as a mild, tolerable warming sensation with no downtime after treatment.
2.3 Why Deep Penetration Matters for the Upper Cervical Spine
The alar ligaments lie beneath the suboccipital muscles, the posterior atlanto‑occipital membrane, and layers of fascia. A low‑power laser simply cannot deliver enough photons to this depth to stimulate a biological response. Class IV lasers overcome this barrier by using higher energy density while keeping treatment times short. The near‑infrared spectrum also faces less scattering and absorption by water and hemoglobin, meaning more light reaches the target. This depth advantage makes Class IV laser uniquely suited for craniocervical junction injuries that were previously treatable only with injections or prolonged rest.
3. Why Class IV Laser Makes Sense for Boxers and Rugby Players
For combat and contact athletes, time away from training means lost conditioning, lost competitive edge, and sometimes lost contracts. Class IV laser therapy fits the unique demands of these athletes in ways that other treatments cannot.
3.1 No Downtime Between Training Sessions
A boxer cannot afford to miss a week of sparring. A rugby player cannot sit out two weeks of contact drills. Class IV laser sessions take only 8 to 15 minutes and require no recovery period. Athletes walk out of the clinic and return to practice the same day. This is a critical advantage over corticosteroid injections, which often require a week of rest to avoid tendon rupture, or over surgery, which takes months of rehabilitation. Laser therapy respects the athlete’s schedule, not the other way around.
3.2 Drug‑Free Pain Control Without Side Effects
Many athletes hesitate to take anti‑inflammatory medications because of potential stomach issues, kidney stress, or masking pain that serves as a warning signal. Opioids are out of the question for anyone subject to anti‑doping rules. Class IV laser provides local, targeted inflammation reduction without a single pill entering the bloodstream. There are no drug interactions, no drowsiness, and no risk of a positive doping test. For boxers and rugby players who undergo random testing, this clean profile matters tremendously.
3.3 Treats the Ligament, Not Just the Symptoms
Muscle relaxants and painkillers only mask the problem. Ice and heat offer temporary relief but do not repair torn collagen fibers. Class IV laser directly stimulates the fibroblasts inside the ligament to produce new collagen. It addresses the root cause of the instability, not just the secondary muscle spasms or headaches. Once the alar ligament heals, the athlete returns to sport with genuine structural improvement, not just a temporary reduction in pain. This distinction makes laser therapy a true healing modality rather than a short‑term bandage.
3.4 Cumulative Benefits Over a Career
A single alar ligament sprain often indicates that the athlete’s neck has taken multiple smaller insults over time. Class IV laser therapy not only treats the current injury but also helps remodel older scar tissue from previous micro‑traumas. With each treatment course, the ligament becomes more resilient. Many combat sport athletes find that periodic maintenance sessions—once a month or once every few months—keep their upper cervical spine feeling stable and responsive. This turns laser therapy from a reactive treatment into a proactive tool for long‑term neck health.
4. Practical Application for Combat and Contact Athletes
Knowing that Class IV laser therapy works in theory is one thing. Knowing how to use it around a training and competition schedule is another. Here is how boxers and rugby players can integrate laser treatment for alar ligament strains, along with guidance on when laser therapy may not be enough.
4.1 Timing Around Training and Competition
Athletes should avoid treating an acute alar ligament strain immediately before a fight or match. In the acute phase (first 48 to 72 hours after injury), the priority is reducing inflammation. Laser therapy during this window helps limit the spread of inflammatory mediators. Once the acute phase passes, athletes can schedule laser sessions on recovery days or after lighter training sessions. Many sports medicine clinics recommend two to three sessions per week for two to four weeks, depending on injury severity. Never treat the neck immediately before heading into the ring or onto the pitch, as the tissue may feel looser but has not completed healing.
4.2 What to Expect During a Treatment Session
A typical Class IV laser session for the upper cervical spine lasts 8 to 15 minutes. The clinician or physical therapist applies the laser handpiece directly to the skin at the base of the skull, following the line of the alar ligament‘s attachment points. The athlete lies face down or sits comfortably upright. The laser produces no sound and only a gentle warmth. No needles, no medication, no sedation, and no recovery period follow the session. Athletes can return to light training within hours, though heavy contact should wait until the full treatment course finishes.
4.3 Combining Laser with Rehabilitation Exercises
Laser therapy cannot work alone. For full recovery, athletes must perform targeted stabilizing exercises for the deep neck flexors and suboccipital muscles. These muscles take over some of the stabilizing work that the injured alar ligament can no longer perform. Simple exercises include chin tucks performed lying down and isometric holds against a yoga ball. A physical therapist should guide the progression. Athletes who skip this step risk incomplete healing and an early return of symptoms. The laser accelerates the ligament‘s repair, but exercise retrains the neuromuscular system to protect the vulnerable joint.
4.4 When Laser Treatment Is Not Enough
Partial or complete ruptures of the alar ligament may not respond to laser therapy alone. Symptoms that worsen over time despite consistent treatment, ongoing dizziness or visual disturbances, a sensation that the head feels like a bobblehead, or MRI findings showing a full‑thickness tear all suggest more serious injury. In these cases, athletes need consultation with a spine specialist. Options range from prolotherapy to surgical stabilization for the most severe injuries. Laser therapy remains a valuable tool for the huge middle ground of grade 1 and grade 2 alar ligament sprains—those not requiring surgery but also not healing on their own.
Frequently Asked Questions (FAQ)
Q1: Can a Class IV laser completely heal a torn alar ligament?
Complete healing of a full tear is unlikely with any non‑surgical method. However, for mild to moderate sprains (grade 1 and grade 2), Class IV laser therapy significantly accelerates collagen repair and reduces symptoms.
Q2: How many laser sessions will a boxer or rugby player need?
Most athletes require 6 to 12 sessions over two to four weeks. Some return to competition after the initial course, while others need periodic maintenance sessions when symptoms flare.
Q3: Does the treatment hurt?
No. Most athletes feel only a mild warmth where the laser contacts the skin. The treatment is painless and does not require any numbing or anesthesia.
Q4: Can I do neck exercises immediately after a laser session?
Yes. Gentle range‑of‑motion and isometric exercises are fine. However, avoid heavy sparring or contact drills until the full treatment course finishes, as the ligament needs time to remodel.
結論
A boxer‘s jaw and a rugby player’s neck withstand forces that would injure almost anyone else. When those forces exceed the alar ligament‘s limits, the resulting instability can end a career if left untreated. Class IV laser therapy offers a non‑invasive, drug‑free path to healing these deep cervical ligaments. By delivering high‑power near‑infrared light to depths that cold lasers cannot reach, Class IV technology accelerates collagen repair, reduces inflammation, and shortens recovery time. When combined with targeted stabilizing exercises and proper medical guidance, laser therapy allows contact sport athletes to return to the ring or the pitch—not just healed, but stronger and more aware of the small but mighty structures that hold their heads up.
References
ScienceInsights. Alar Ligament Injury: Symptoms, Diagnosis, and Treatment.
https://scienceinsights.org/alar-ligament-injury-symptoms-diagnosis-and-treatment/
RegenCore Method. Understanding Alar Ligament Injury: Symptoms and Treatment Options.
https://regencoremethod.com/understanding-alar-ligament-injury-symptoms-and-treatment-options/
FotonMedix. クラス4レーザー治療: Advanced Solutions for Pain and Inflammation.
https://fotonmedix.com/class-4-laser-therapy-advanced-solutions-for-pain-and-inflammation.html/
Dvorak J, Panjabi MM. Functional anatomy of the alar ligaments. Spine. 1987;12(2):183-189.