
محتويات الصفحة
مقدمة
You feel a dull, aching pain at the base of your skull. It creeps up one side of your head and settles behind your eye. Your neck feels stiff, and turning your head makes the pain worse. This pattern points to a cervicogenic headache—a type of secondary headache where the source of the pain lies in the cervical spine rather than in the head itself. Unlike migraines or tension-type headaches, this condition stems from mechanical dysfunction in the neck. For those who have tried conventional approaches without lasting relief, العلاج بالليزر من الفئة الرابعة offers a non-invasive, drug-free option that targets the underlying cervical structures rather than just masking the symptoms.
1. What Is a Cervicogenic Headache?
A cervicogenic headache produces head pain that originates from the bony structures or soft tissues of the neck. This referred pain happens when you feel discomfort in a part of your body that is different from the actual source. With cervicogenic headaches, the pain you experience in your head truly starts in your cervical spine, often due to an injury, arthritis, a slipped disk, or postural muscle dysfunction such as keeping your head tilted forward over electronic devices for prolonged periods.
1.1 Key Features That Distinguish It from Other Headaches
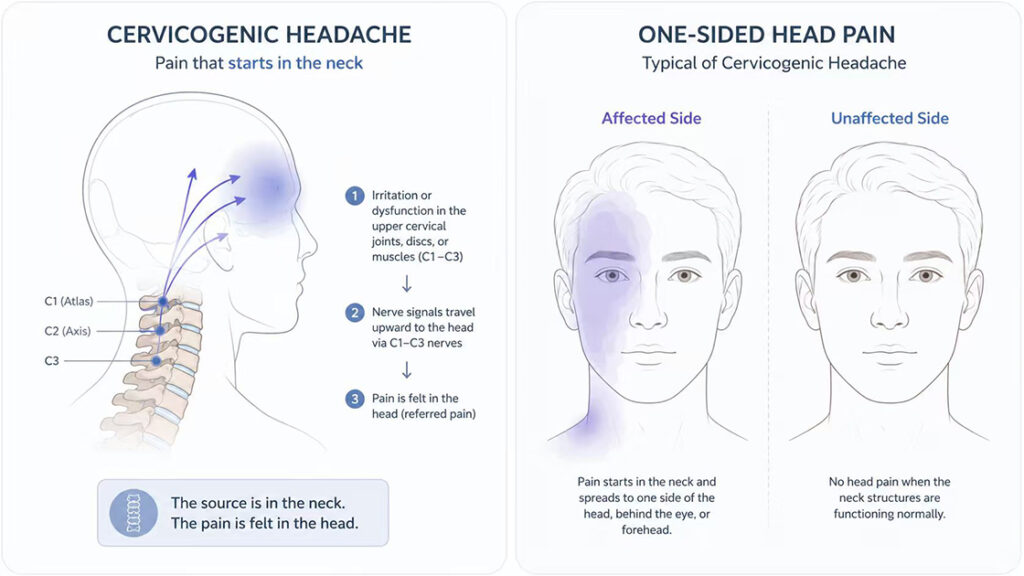
Cervicogenic headaches typically affect one side of the head, and the pain often starts at the back of the neck at the base of the skull before radiating to the forehead or behind the eyes. Limited range of motion in the neck is a hallmark feature, and the headache frequently worsens with neck movement or sustained awkward head positions. Unlike migraines, cervicogenic headaches do not usually cause nausea or sensitivity to light and sound. This distinction matters because treatment directed at the neck often relieves the headache, whereas migraine medications typically do not.
1.2 How Common Is This Condition?
Cervicogenic headaches are less common than migraines or tension-type headaches but still affect a notable portion of the population. Studies suggest that cervicogenic headaches account for up to about 15–20% of chronic headaches. In the general population, the prevalence ranges from 0.4% to 4% among those who experience headaches. Among patients who have persistent headaches, the numbers climb higher, and the condition appears to be more common in women. The average age of onset sits in the early thirties, although many individuals do not seek treatment until their late forties. This delay often means that the underlying cervical dysfunction has been progressing for years.
2. Why Does the Neck Cause Head Pain?
Understanding the connection between the neck and head requires a look at the nerve pathways that link these two regions. The upper cervical spine houses nerves that transmit signals directly to areas of the head and face. When structures in the neck become irritated or dysfunctional, those nerve pathways carry pain signals upward, creating the sensation of a headache that feels like it originates in the head.
2.1 The Upper Cervical Nerves Involved
The spinal nerves C1, C2, and C3 innervate the bony structures and soft tissues of the upper cervical spine. These same nerves also carry sensory information to parts of the skull, face, and scalp. When a problem arises in the atlanto-occipital joint, the facet joints, the intervertebral discs, or the paraspinal muscles at these upper levels, the irritation travels along the C1–C3 nerve pathways. The brain interprets this incoming signal as coming from the head, even though the actual source remains in the neck. This phenomenon explains why a stiff neck can cause a headache and why treating the neck often relieves the head pain.
2.2 Common Underlying Causes
Several conditions can trigger cervicogenic headaches. Cervical disc pathology, such as a herniated or degenerated disc, can irritate nearby nerve roots and produce aseptic inflammation within the nerve fibers responsible for transmitting pain. Trauma, particularly whiplash from motor vehicle accidents, frequently initiates chronic cervicogenic headache patterns. Arthritis of the upper cervical facet joints represents another common cause, as joint inflammation and degeneration generate persistent pain signals. Postural muscle dysfunction, sometimes called “tech neck” or “text neck,” from prolonged forward head posture while using smartphones, tablets, or laptops, places sustained mechanical strain on the upper cervical structures and can trigger headache symptoms in susceptible individuals.
3. How Class IV Laser Therapy Works at the Cellular Level
Class IV laser therapy uses specific wavelengths of light, typically in the near-infrared spectrum, to deliver photonic energy into deeper tissues. This process, known as photobiomodulation, does not heat or damage the tissue. Instead, it triggers beneficial biological responses at the cellular level that support tissue repair and pain modulation.
3.1 The Photobiomodulation Process
When photons from a Class IV laser reach the target tissues, mitochondria within the cells absorb the light energy. This absorption stimulates the production of adenosine triphosphate (ATP)—the primary energy currency of the cell. A temporary increase in ATP availability supports various cellular functions, including membrane transport, protein synthesis, and waste removal. In addition, photobiomodulation influences the activity of transcription factors that regulate genes involved in the cellular response to mechanical stress and inflammation. These molecular events occur without any thermal injury to the surrounding structures.
3.2 Effects on Inflammation and Local Circulation
The laser energy reduces the levels of pro-inflammatory markers such as prostaglandin E2, interleukin 1β, and tumor necrosis factor α. This modulation of the inflammatory environment helps the body transition from a chronic, unresolved inflammatory state toward a more constructive healing process. Additionally, Class IV laser therapy increases local microcirculation by promoting the growth of new blood vessels—a process called neovascularization. Better blood flow brings oxygen and nutrients to the injured tissues while carrying away metabolic waste products that can accumulate in chronically dysfunctional areas.
3.3 Pain Modulation Mechanisms
The analgesic effects of photobiomodulation involve multiple pathways. The laser energy can influence how pain receptors transmit signals to the spinal cord and brain, effectively reducing the perception of pain without the use of pharmaceuticals. Some evidence indicates that photobiomodulation increases serotonin levels and selectively inhibits the activity of small-diameter nerve fibers responsible for transmitting pain signals. This combination of anti-inflammatory and neuromodulatory effects makes Class IV laser therapy particularly suitable for conditions like cervicogenic headache, where both tissue inflammation and nerve irritation play roles.
4. Clinical Evidence for Class IV Laser in Cervical Spine Conditions
A growing body of research supports the use of high-intensity laser therapy for neck pain and related cervical spine disorders. Systematic reviews and clinical trials have examined both pain reduction and functional improvement.
4.1 Systematic Review Findings
A systematic review and meta-analysis evaluated the effects of high-intensity laser therapy on pain, disability, and range of motion in patients with neck pain. The review included multiple randomized controlled trials and found statistically significant improvements in pain intensity, cervical extension range of motion, and neck disability scores in favor of high-intensity laser therapy. The evidence, assessed as moderate in quality, indicates that high-intensity laser therapy demonstrates effectiveness when added to other physical therapy interventions, particularly therapeutic exercise. The review specifically noted that the most favorable outcomes occur when the therapy addresses myofascial pain, cervical radiculopathy, and chronic neck pain.
4.2 Comparative Effectiveness Studies
A randomized controlled trial comparing Class IV laser therapy with therapeutic ultrasound in patients with chronic neck pain found that Class IV laser produced significantly greater improvement across all outcome measures. The laser group showed more substantial reductions in pain scores and greater improvements in functional status compared to the ultrasound group. Another clinical trial protocol specifically examines Class IV laser therapy for cervicogenic headache in young adults, anticipating that the laser intervention will lead to significant reductions in both neck pain and headache intensity.
5. Integrating Class IV Laser Therapy into a Comprehensive Approach
Class IV laser therapy works most effectively when individuals also address the factors that contributed to their cervicogenic headache in the first place. It is not a standalone solution but rather a supportive intervention that works alongside sensible self-care strategies.
5.1 Postural Awareness and Ergonomics
Given that prolonged forward head posture from electronic device use contributes to cervicogenic headaches, modifying daily habits can reduce mechanical strain on the upper cervical spine. Positioning computer monitors at eye level, using a headset for phone calls instead of cradling the phone between the ear and shoulder, and taking frequent breaks from looking down at smartphones all help maintain a more neutral cervical alignment. Simple awareness of head position throughout the day can complement the tissue-level effects of laser therapy.
5.2 Complementary Self-Care Strategies
A few practical habits can support the healing process. Gentle, pain-free range-of-motion exercises for the neck performed several times daily help maintain joint mobility and prevent stiffness from setting in. Using a supportive pillow that keeps the cervical spine in a neutral position during sleep reduces overnight strain on the upper joints and muscles. Applying a warm compress to the neck before laser sessions may relax superficial muscle tension and improve tissue pliability. These small adjustments create a more favorable environment for the cervical tissues to respond to the laser therapy.
FAQ
Q1: What exactly does a cervicogenic headache feel like?
The pain typically starts at the back of the neck or base of the skull and spreads upward to one side of the head, often settling behind the eye or in the forehead. Neck movement or sustained head positions often make the pain worse.
Q2: How is a cervicogenic headache different from a migraine?
Cervicogenic headaches originate from a problem in the neck, whereas migraines come from within the nervous system. Cervicogenic headaches usually lack the nausea, vomiting, and light sensitivity that commonly accompany migraines.
Q3: How many Class IV laser sessions are typically needed?
A course of treatment often involves six sessions delivered on alternate days, although the exact number depends on the severity and chronicity of the condition. Some individuals notice improvement after two or three sessions, while others benefit from a longer series.
Q4: Can Class IV laser therapy be combined with other treatments?
Yes. Laser therapy works well alongside physical therapy, exercise, postural training, and other non-invasive modalities. Clinical evidence suggests that the best outcomes occur when laser therapy is added to other active interventions.
Q5: Is Class IV laser therapy safe for someone with a history of neck surgery?
In most cases, yes. However, anyone with previous neck surgery or implanted hardware should consult their physician and inform the laser practitioner before beginning treatment.
الخاتمة
Cervicogenic headaches arise from a problem in the upper cervical spine, but the pain radiates to the head, creating confusion for those who struggle to find lasting relief. Unlike migraines or tension-type headaches, these secondary headaches respond to treatments that address the underlying neck dysfunction. Class IV laser therapy, operating through the principles of photobiomodulation, offers a non-invasive, drug-free approach that reduces inflammatory markers, improves local microcirculation, and modulates pain signaling pathways. Clinical evidence supports its effectiveness for chronic neck pain and related cervical spine conditions, particularly when combined with appropriate exercise and postural strategies. For individuals who have spent years searching for answers to their persistent headaches, Class IV laser therapy represents a promising option that treats the neck to heal the head.
References
Cleveland Clinic – Cervicogenic Headache
https://my.clevelandclinic.org/health/diseases/cervicogenic-headache
Harvard Health Publishing – A Headache That Starts in Your Neck
https://www.health.harvard.edu/pain/a-headache-that-starts-in-your-neck
StatPearls – Cervicogenic Headache
https://www.ncbi.nlm.nih.gov/books/NBK507862
Sahani A, Sharma S – Impact of Class IV LASER Therapy and Conventional Exercise on Young Adults with Cervicogenic Headache
de la Barra Ortiz HA et al. – A systematic review and meta-analysis on the effectiveness of high-intensity laser therapy in the management of neck pain
https://pubmed.ncbi.nlm.nih.gov/38709332
Shrestha D, Sharma S – Comparison of the clinical effectiveness of Class IV Laser therapy and therapeutic ultrasound in patients with chronic neck pain
https://www.semanticscholar.org/paper/80244caf88efc920057c9bd586879167c610e43f